Narendra Jana
Email: narenjana@narenjana.com
Email: narenj5@protonmail.com
The course of events are explained as below:
1. The first is clinical assault that took place between March 11th and March 16th to 17th 2018 in Charity Hospital Mitte and Charity Hospital Virchow (this page explains the assault).
The assault is followed by medical treatment in Bunderswehrkrankenhaus Berlin on March 17th and 18th 2018 followed by medical treatment under Dr. med. Stefanie Klaffke (also explained in the end of this page).
2. The second is medical fraud in Labor Berlin (which is part of Charity Hospital) for a test ordered/completed by Dr. Daniela Bermphol in Charity Hospital. The fraudulent medical test was used to assault the patient on March 11th and March 16th to March 17th in Charity Hospital Emergency Room.
The link is given here: https://narenjana.com/police/germany/labfraud
3. Radiological fraud in Riga, Latvia that demonstrates the clinical fraud in Dr. Pia Schumacher's statements to assault me in this setting.
The link is given here: https://narenjana.com/police/germany/mrifraud
Assault Berlin, Germany March 11th and March 16th to 17th 2018:
Assault by Dr. Benjamin Hotter on March 11th
The compiled data in this listing gives clear evidence of assault in a clinical setting using flasified medical data. In this case clear intent to physically harm the patient with video and audio evidence.
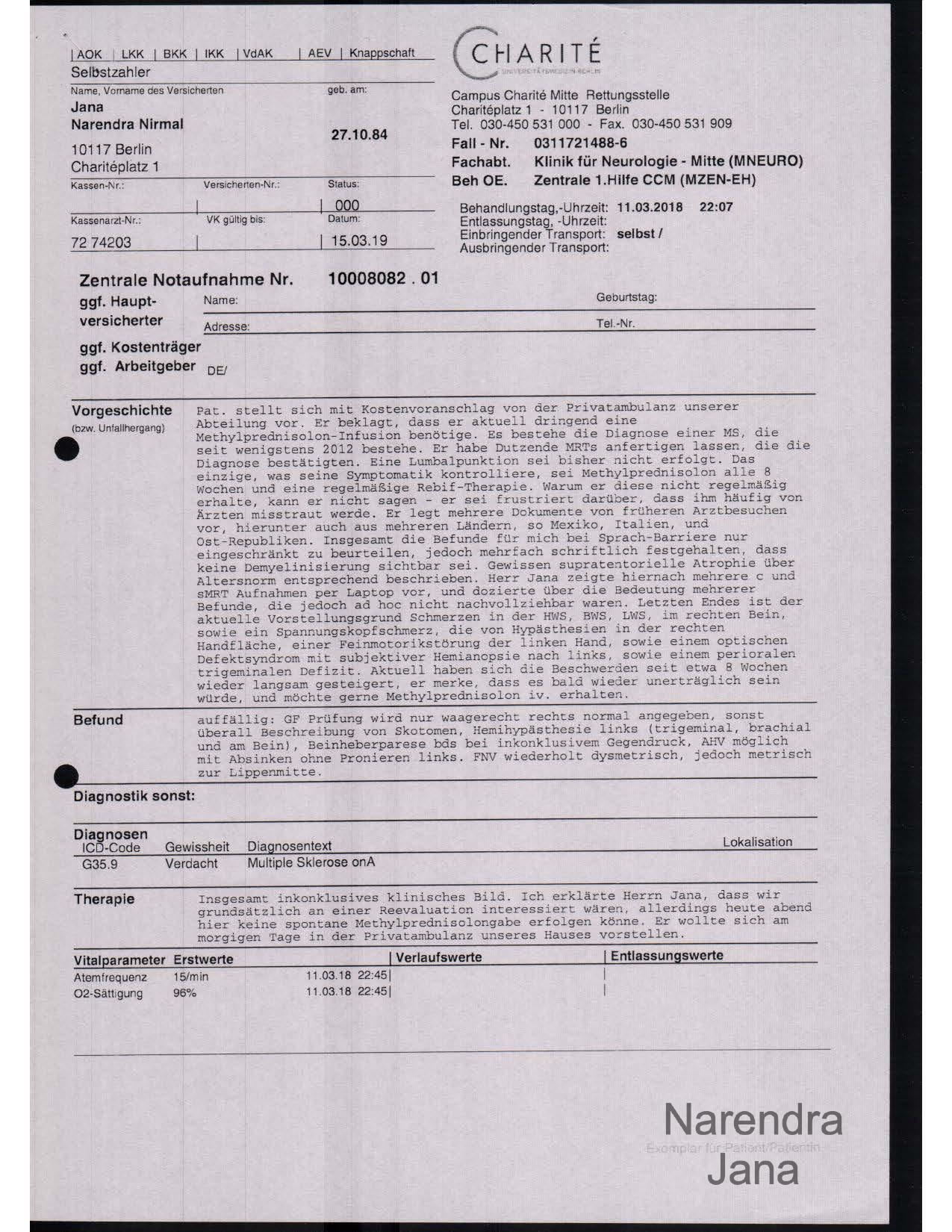
On March 11th 2018 after my condition (Mutiple Sclerosis) got rapidly getting worse. I decided to go the ER room in Charity Hospital, Berlin.
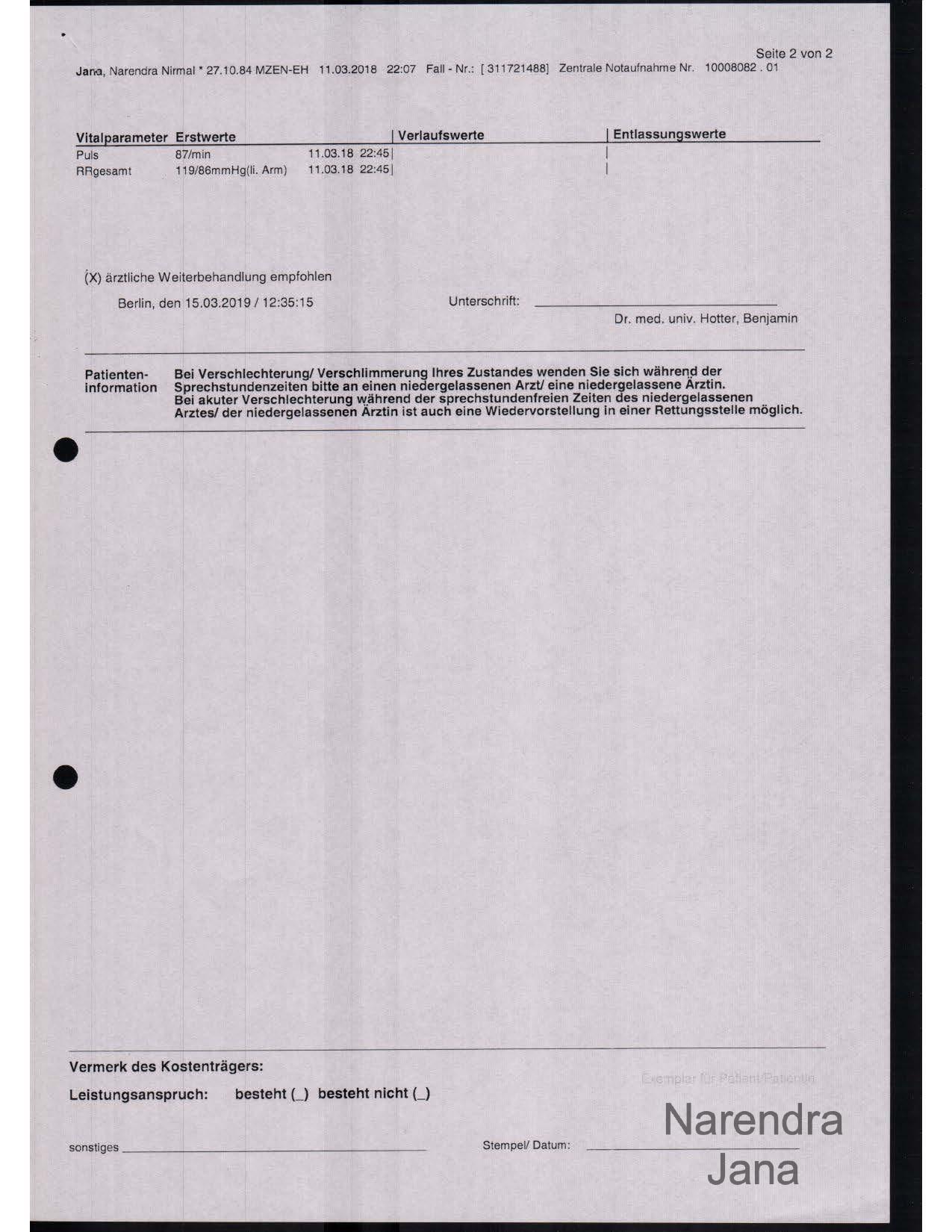
Discharge Report (Dr. Benjamin Hotter) from March 11th 2018 Charity Mitte:
|
|
|
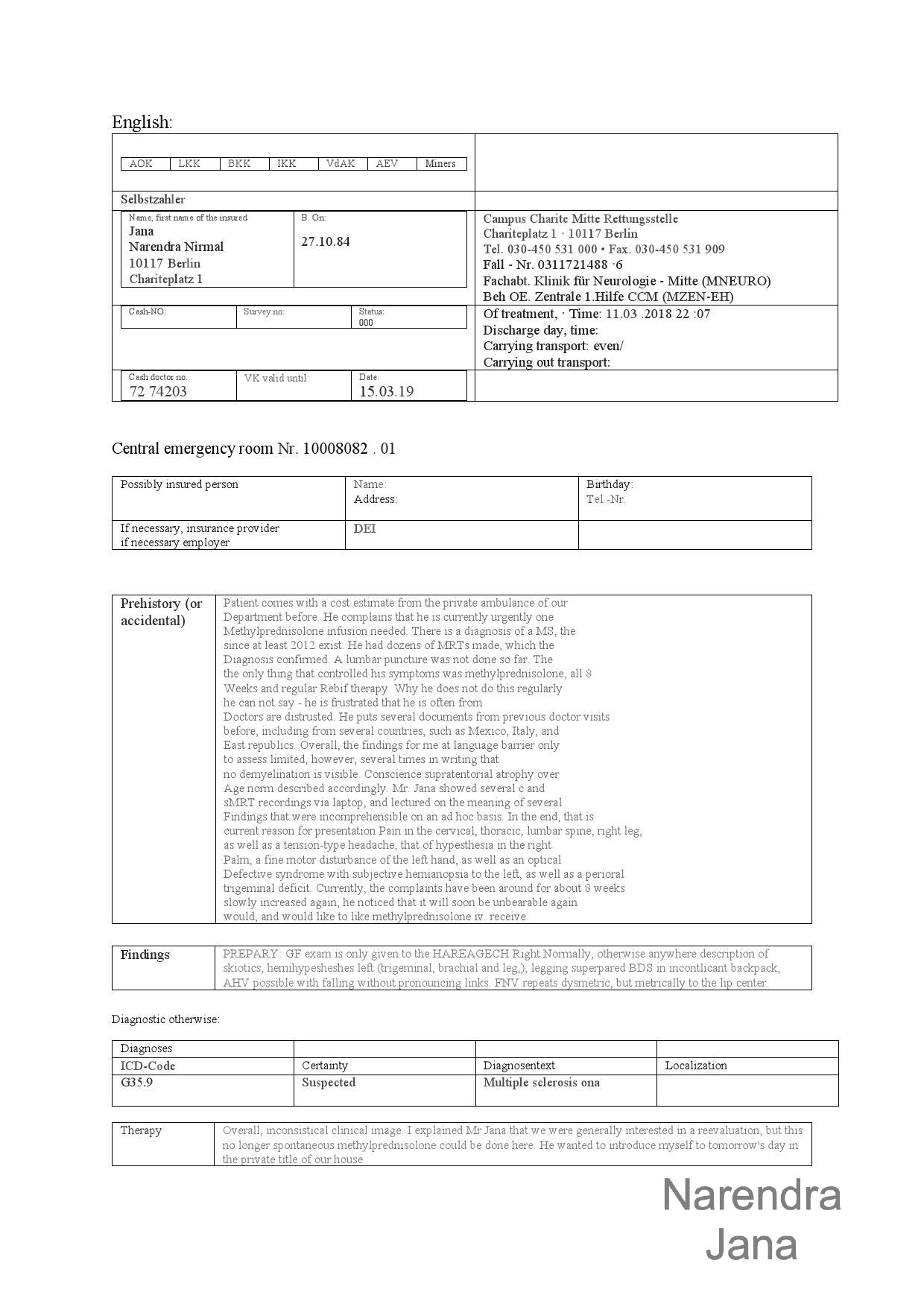
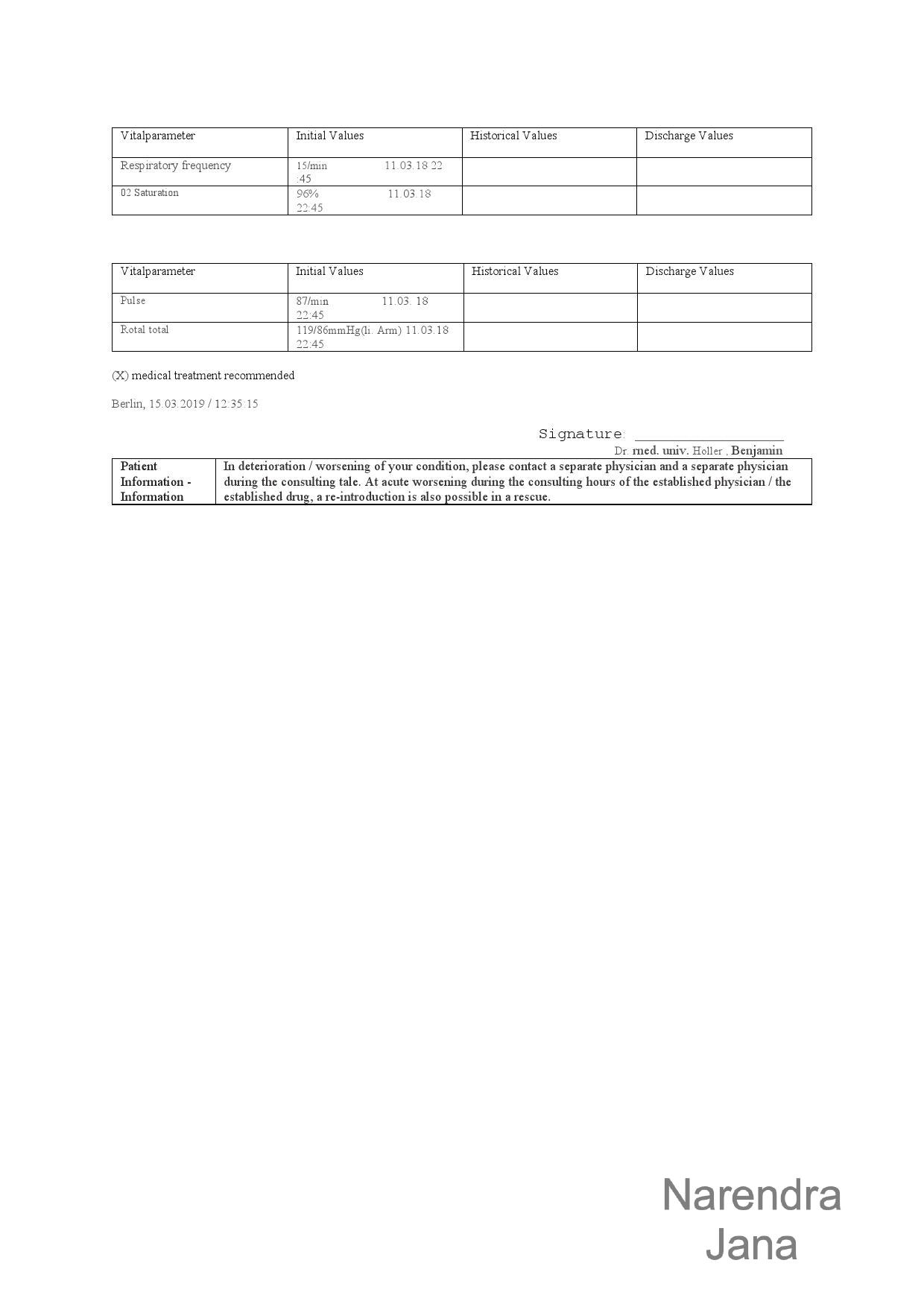
English translation:
|
|
The physician denied medical treatment citing that "the hospital didn't have any beds". The clinician falsified his clinical report.
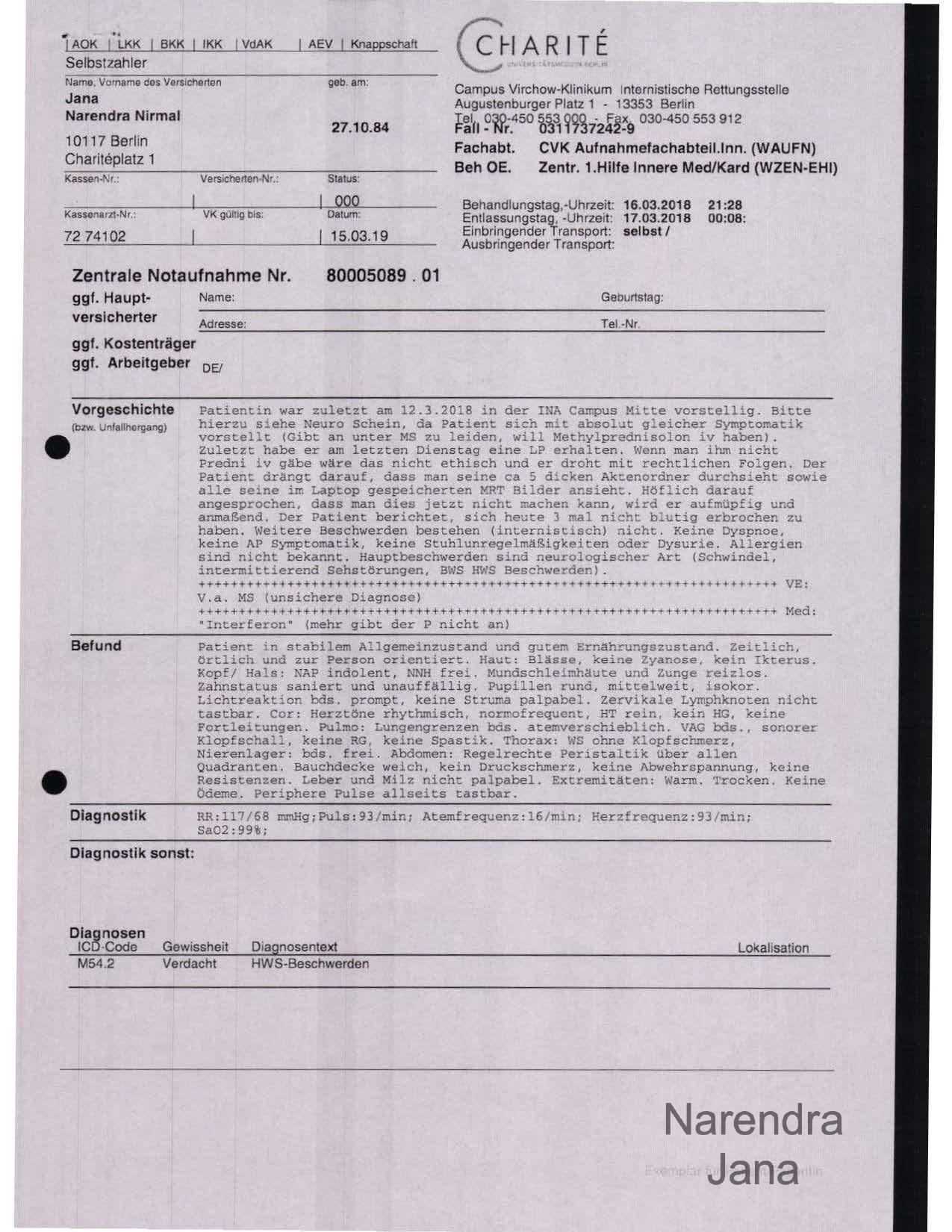
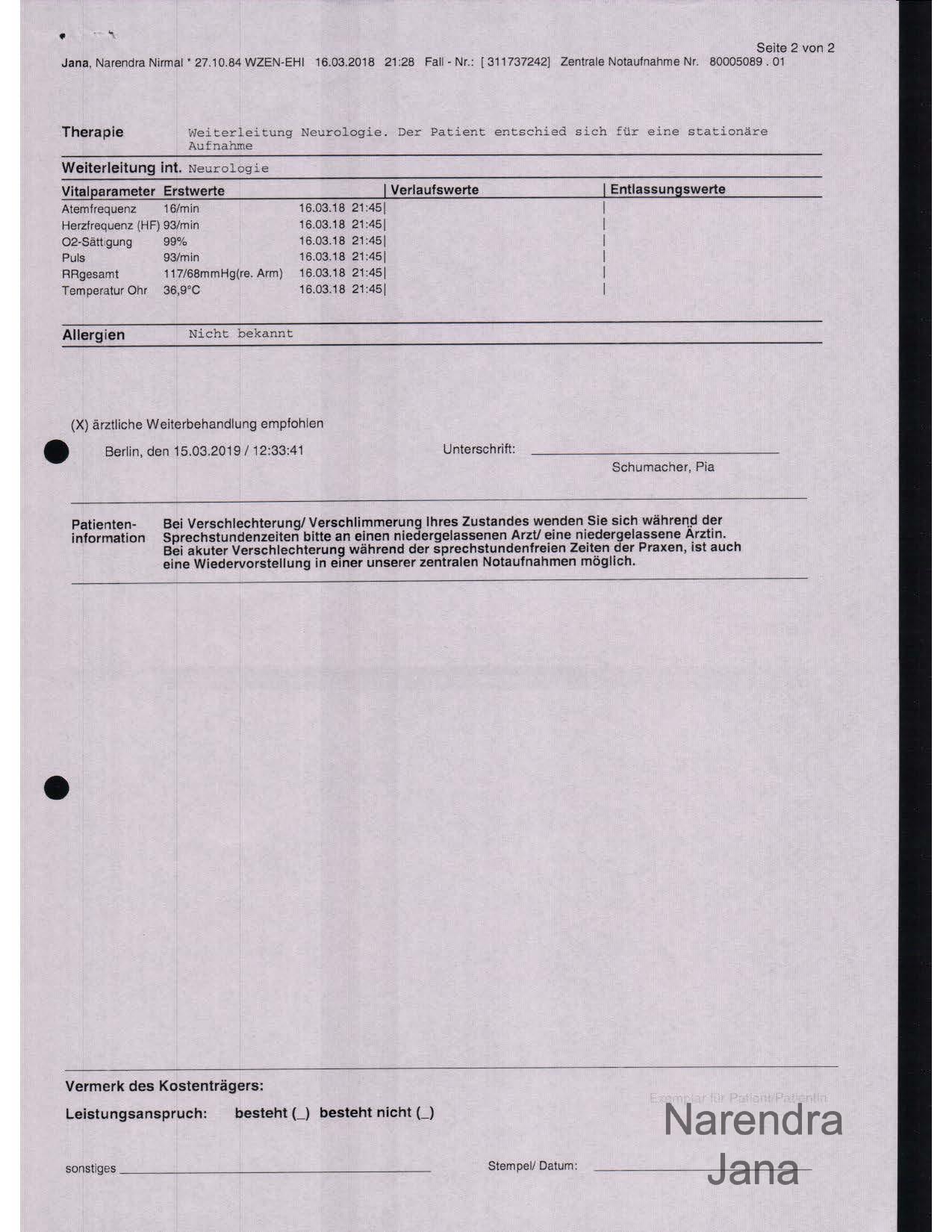
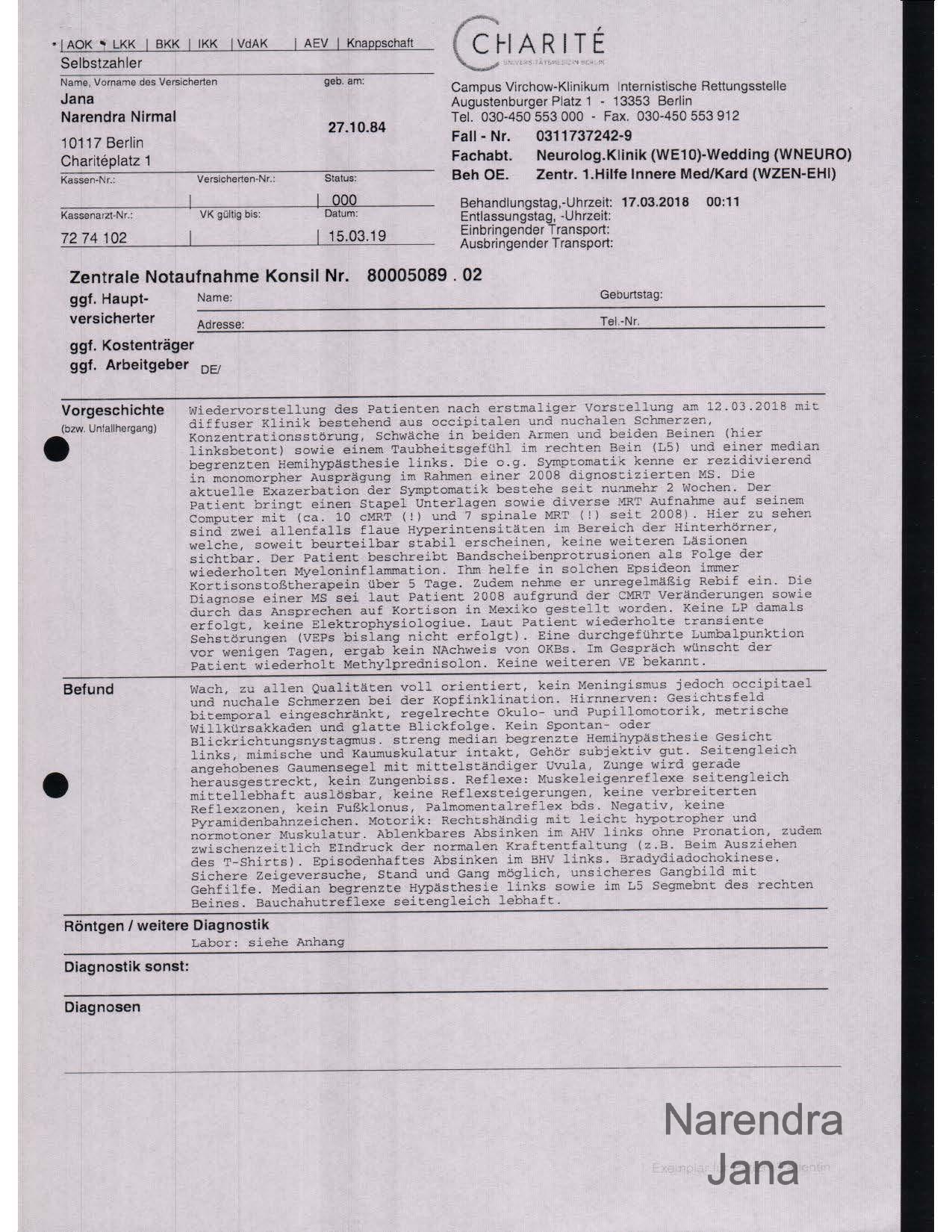
Clear Assault by Dr. Pia Schumacher and Dr. med. Kaspar Streitberger in a Emergency Room Setting and then wardroom setting on March 16th and 17th 2018
Clinical Report from March 16th 2018 Charity Virchow
(clinical report is against clear clinical presentation):
|
|
English Translation:
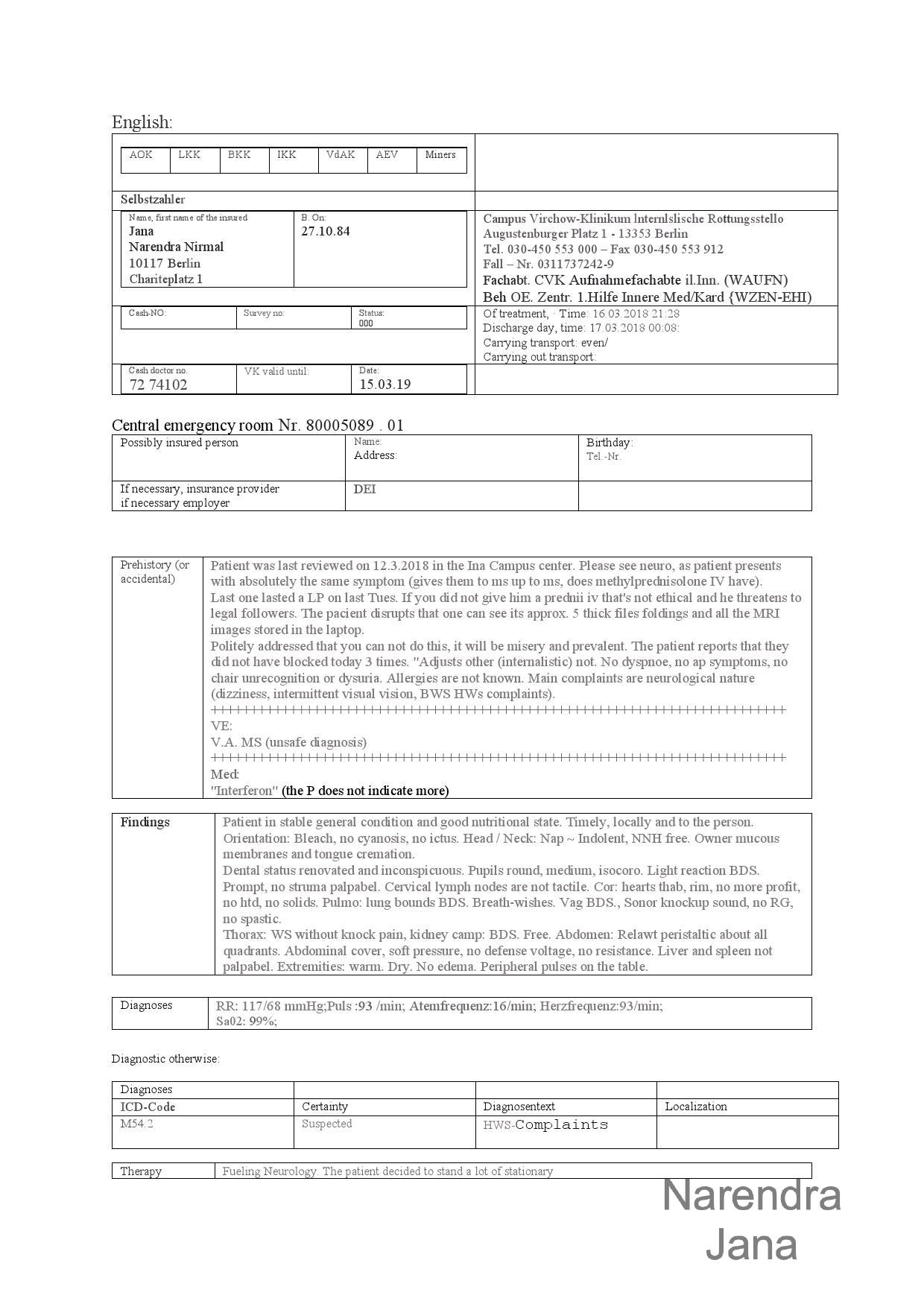
|
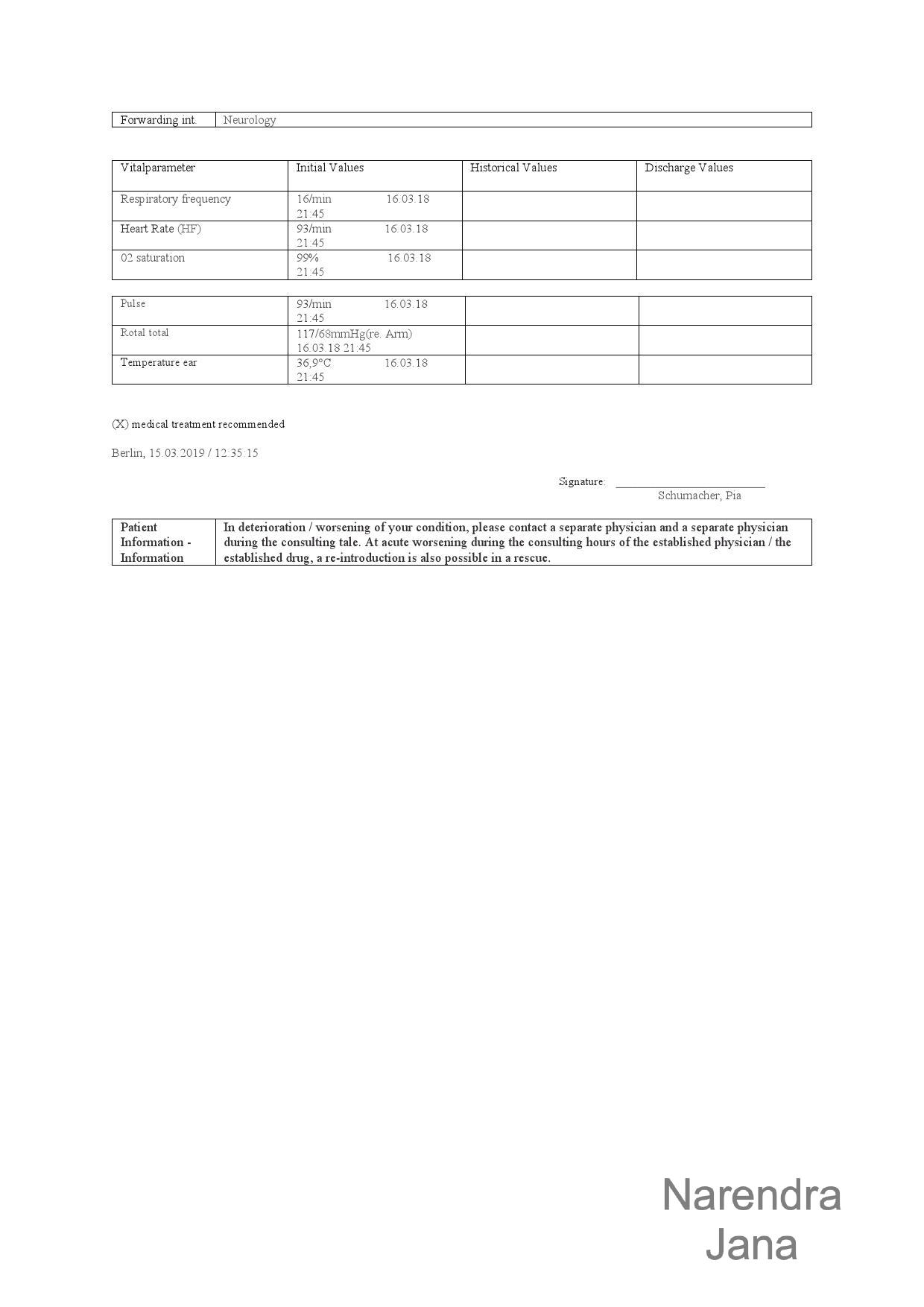
|
First Conversation with Dr. Pia Schumacher:
Dr. Schumacher's First Conversation Transcript:
Pia: Ok, Mister Jana.
Pia: No I would not leave your laptop there, I would take your things.
Pia: Sit here.
Pia: So, where was the Multiple Sclerosis diagnosed?
Me: The first place was, lets see. When did I start taking Rebif? That was in [2017] in Mexico.
Pia: And what was the clinic?
Me: It was an outpatient doctor. His name is Dr. Hugo Baez Navarate.
Pia: No, but what was the clinic?
The clinical symptoms that led to the diagnostics?
Me: Huh, well the same. Or almost about the same thing. A lack of physical feel in my peripheral extremities. Huhh, lack of feeling in my face my midface, my lips. And huh....
Pia: So you have MRI scans with you?
Me: Yup I have the MRI scans with me.
[by peculiarity the doctor appears to know that I have my MRI scans with me without any mention or preemption. I believe his objective was to make comments on the MRIs that were medically unsubstantiated to uphold clinical fraud]
Pia: Could you show it to me.
Me: I also have the medical reports from the ER appointments as well so I have both.
The typical presentation is, what is it.
Pia: Its always the same, there is no change.
[this is doctor Pia's next imbecilic argument, that since the relapses in MS presents in the same pattern they shouldn't be treated to prevent further neurodegeneration, its imbecilic and causes harm to a patient with progressive neurodegeneration]
Me: There is a usually a massive headache there are lesions in the upper cervical column at that point and that would create both the headaches and then nausea vomiting and then there are peripheral pains which can become excruciating. Its almost unbearable at that point so. I have some of the MRI examples, there are actually quiet a few.
There are almost 10, 15 MRIs done.
Pia: 10, 15 MRIs?
Me: So, I did it specifically to show relapse and remission and then I had the radiologist do a comparison.
So that shows posterior brain [lesions], and you can see.... Its mostly the occipital region. And what typically happens is that.... if
Pia: So where is the lesion?
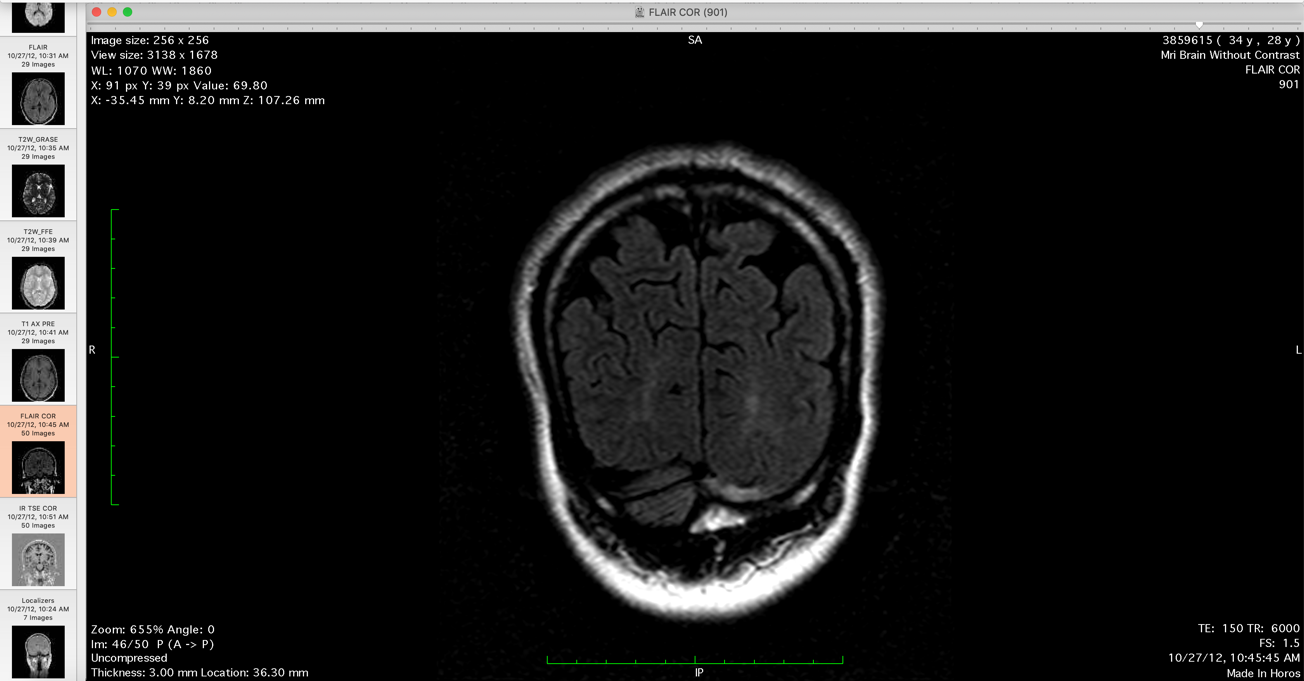
[these are the clear lesions shown to Dr. Pia, which he deludedly professes not to be able to see its clinical fraud in statement]
Me: Keep going back. So there you go, these intensities here.
Pia: Lets look at the transversal slides.
Me: Its depends on the, what I did is that I had the radiologist do a comparison of the different MRIs and then he noted where these intensities.
Pia: So these are the newest ones.
Me: No these aren't the newest.
Pia: Show me the newest.
Me: So, this is the new, newer. This would show the posterior intensity sometime it will show some central intensity....
Pia: Contrast enhanced in any one of time? [Dr. Pia makes a misstatement]
Me: Hmm, they have. The contrast is the T1 images hmm, but....
Pia: Do you have any spinal lesions?
Me: Yup, I do as well. I have the spinal MRI, just have to move the mouse to the right.
That's a.... that wouldn't.... you can go to the next series.
I can show you where.
Pia: Which one is this?
Me: You can go next. Hold on, there is actually 4.
So.... So what happened is that you could do a comparison of the MRIs.
There is some posterior atrophy here and then these are over sequential MRIs.
It will show some intensity in the posterior brain.
Pia: Do you, have you ever heard of the McDonald criteria for MS?
Me: You would have to have 2 relapses and a....
Pia: You have to have supratentorial and infratentorial lesions and you have to have atleast one contrast enhancement or clinical relapses in terms of new, that's what I am saying in terms of new clinic. [clinical symptoms]
[at this point in the clinical course of MS I am well beyond McDonald's
criteria presenting with progressive neurodegeneration along the cervical spine
which Dr. Pia tries to lie about, the evidence of clinical fraud with video to
demonstrate fraud negates the McDonald's criteria since the formation of new
lesions or neurodegeneration is repeatedly attempted to be erased (with video
evidence of fraud taking place). A clear example of evidence in radiological fraud is given below
His statement becomes additively more impossible when he makes a gross lie about the features of progressive neurodegeneration that equate to fraud in clinical statement].
Pia: That is what I am saying, in terms of new clinic. Have you ever had a vision loss?
Did you ever have visual evoked potentials?
Me: Its been recorded in a clinical setting, so....
If there is a visual loss then I usually end up in the hospital and then so this is one noted point. Intermittent vision loss was a point noted in a ER setting sometime last year. It responds quiet well to just giving methylprednisolone. And then both the neurologists and the attending nurses there noted that my visual returned just by giving steroids.
That was....
Pia: Did you have ever had proof in terms of contrast enhancement of the visual nerve or the optical nerve or the visual evoked potentials? Did you ever have that?
Me: I didn't do the visual evoked potentials.
Pia: Why was that never done?
[the patient is in asylum due to the ER and outpatient doctors in former instances refusing diagnostics to hide the disease pathology, soon after this ER appointment all the evidence for of Visual Evoked Potentials and contrast enhancement of the visual nerve to show optic neuropathy was demonstrated with explicit detail, but Dr. Pia didn't need these tests. He commits assault simply by evidence given to him and the clinical fraud committed within the same Charity Hospital using a falsified lumbar puncture test report by Dr. Bermphol]
Me: I don't know but..... Hmm there is a lesion directly in the occipital lobe, it wouldn't really require. It might not be the optic nerve [it was eventually demonstrated to be the optic nerve]. You can go to the.
Pia: Do you have that image too?
Me: Hmm....
Pia: So you don't have any evidence....
Me: Oh yea, that particular series. But what I did was I did a comparison of brain MRIs and I had the radiologist basically compare....
He compared 4 brain MRIs in this series. He compared the MRI with the 2012 MRI and then 2017. So he is basically comparing 4 MRIs the 20 and.... last year January that are no intensities in the occipital lobes as there are in the 2012 or in the 2....
Pia: So it didn't change
Me: Otherwise there is change in the occipital lobe after the 2010. So these two MRI series here they both have signal intensity changes in the posterior part of my brain.
Pia: Its the same lesion, we are talking about the same lesion.
[this is where Dr. Pia defines intent in clinical negligence (assault) is clear, he is trying to furhter the patients condition by withholding medications to gain lesions (that cause neurological damage) while making medical misstatements and using falsified medical data]
You have not gained any lesion. See, I am kind of questioning the diagnosis to be honest.
Me: Its more what medications.
Pia: We did the spinal tap. And we did not find Oligoclonal bands. We did not.
[Dr. Pia is citing the fraudulated LP test done two days before in Charity Hospital by Dr. Daniela Bermphol, the medical test is frauduluated as
explained in the link below:
The link is given here: https://narenjana.com/police/germany/labfraud
the test result is available well before the length of time required to do electrophoresis for the test, so Dr. Pia is citing clinical fraud to assault in the same medical institution to physically harm the patient; which matches his former statements in the same setting]
Me: The results aren't in yet. Or else....
Pia: I just saw the results.
[The test result is available well before the length of time required to do electrophoresis for the test, its avaliable in two days when it takes 2 weeks to do]
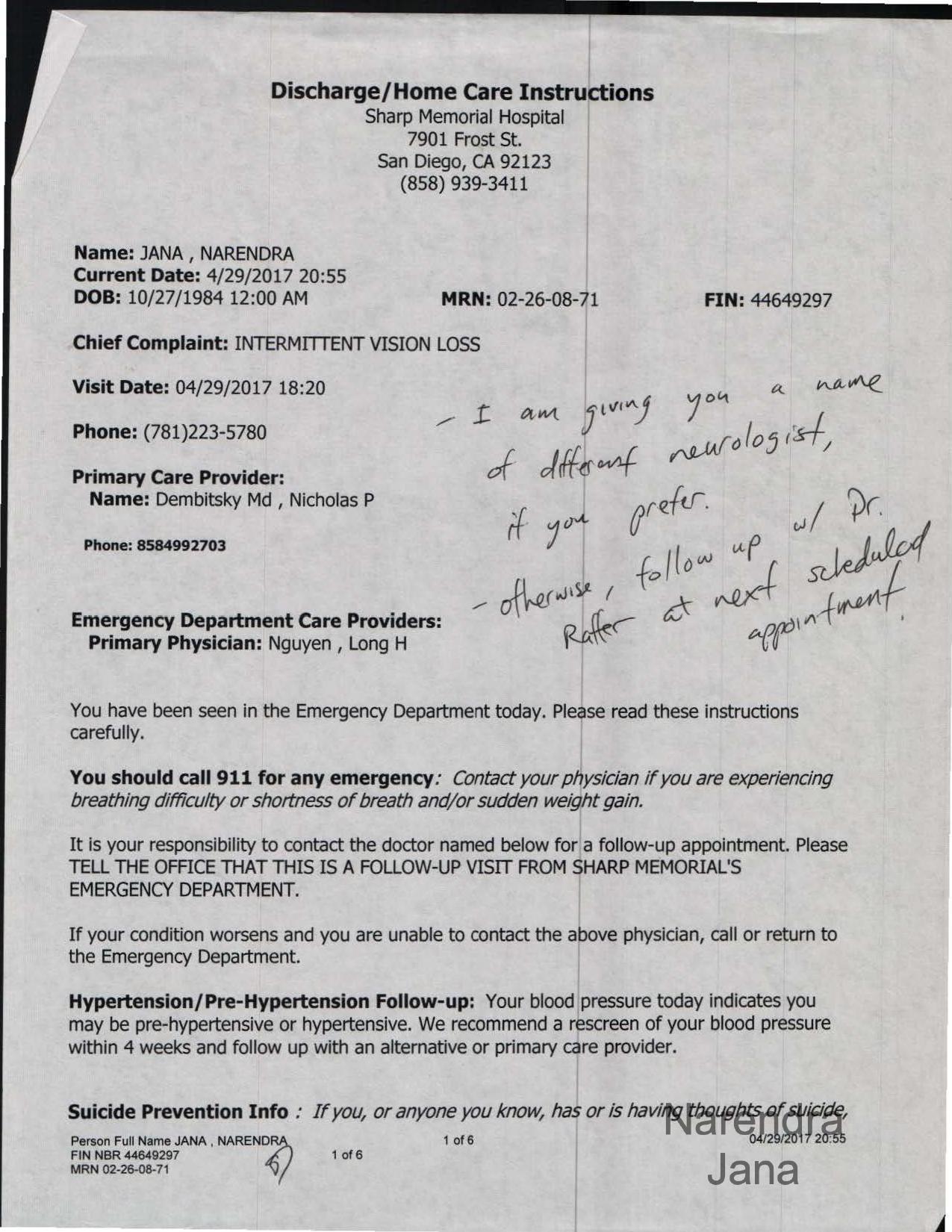
Me: Its definitely fabricated. Because you can see the intensity directly in the..... What is it..... Because you can see the intensities or the neurodegeneration present directly in the cervical column.... and....
Pia: But that's not.. that's not multiple sclerosis..
[at this point Dr. Pia's intent in assault becomes grossly apparently, you would could use another instance of medical fraud to substantiate the clinical fraud in Dr. Pia's statement. The video given below shows a radiologist erasing evidence of the progression of neurodegeneration in multiple sclerosis and negates Dr. Pia's statement with explicit evidence]
Me: Or you could see it in this series here. So you could see it in this series here. You could see some intensity here. This is the reason why I did repetitive MRIs as well. So you can see that is a repetitive intensity....
Pia: Where is the transversal slide of this.
[this is the frauduluated MRI series that Dr. Pia tries to lie about again to uphold subsequent fraud]
Me: This transversal slide wasn't actually wasn't actually done. So what I did is hummm....
There is a transversal slide but there is a.... it wasn't a complete series. And I had to question the radiologist for why she didn't include a complete series.
So you can actually how much we have. We have it from here to here. But we don't have the rest of it.
[this is the MRI series shown below where clinical fraud is taking place in the video, Dr. Pia replicates the same clinical fraud with verbal statement, thats assault with clear evidence in both cases]
Pia: Can you, can you enhance the intensity?
Me: So we only have it from this section to this section. Its no significant, hmmm. Huh, I have the full series in the next MRI image.
So I have the full series in, if you couldn't see it here. So this is why I did repeated MRIs specifically so that.... the next thoracic you can see.
But the point is that it always responds to the medications. So....and in this MRI you can see the central intensity in the axial region [plane].
And that's why, there you go.
[Dr. Pia's statements become stranger as he tried to defend clinical fraud and subsequent assault now]
Me: So the closet you get to the same region.
Pia: So are you taking about this as being a lesion, no that's the central canal its not a lesion.
[Dr. Pia mis typify central intensities that cause neurodegeneration]
Me: It depends on which series you see but it was determined that that's basically it.
Pia: So where is, where is the.... [stutters at a lack of a defense] the neuroradiologist statement.
Me: I only have the MRI series for this.
Or its not there....
This is also another example here.
This is lower lumbar, which describes some of the symptoms. Here there are signs of neurodegenerative changes [from repeated central inflammatory episodes].
Pia: But this has nothing to do with multiple sclerosis.
[Dr. Pia doesn't feel that long term neurodegeneration has anything to do with multiple sclerosis which is what causes secondary progressive Multiple Sclerosis]
Me: It responds to both methylprednisolone and what happened is that the reason why its show that its MS is that its by the drug response.
It was repeatedly given in the ER appointment and then..... huh.
Pia: Well....
Me: These are definitely, because all the MRI images, everything substantiates and drug response also substantiates.....
Pia: There is MR of the cervical and thoracic spine and there is no signs of demyelination.
[this is with evidence of radiologist erasing MRI series images or the thoracic, thus demonstrating Dr. Pia's statements in clinical fraud. Dr. Pia is trying to hide MS in statement (lying) and the radiologist is literally trying to hide the image that shows demyelination]
Me: That's in one series but it will show up in another series thereafter. And that's kinds of
Pia: Well they did the T2, the T1, the T2 Fat Sat imaging. I mean..
Me: So these are clearly very clear lesions in the MRI series but it also responds directly to the medications as well so there is a situation where....
Pia: Wait a minute we are talking about totally different things here. We are taking about. I mean im.... see the multiple sclerosis does inflammation of the brain and the myelin. It does not have anything to do with the spine. Its just not it.
Me: Since when....
Pia: We are talking about, this is bone and this is disk. And this has nothing to do with MS.
[Dr. Pia's statements are now completey nonsensicle. He becomes aggressive; this is clinical fraud, there is no spine pathology; his statements are now desperate clinical fraud to assault the patient with progressive multiple sclerosis. The video of radiological fraud demonstrates Dr. Pia's clinical fraud. The image below and the medical journal comparison shows the fraud in Dr. Pia's statement of "disk" pathology]
Pia: We are talking about the myelin here. See and this has no signs of....
[now I had to educate Dr. Pia about how MRIs work to show the clinical fraud in his statement]
Me: T2 inflammation only shows up in T2 images because you are subtracting the CSF fluid [from the image series]. So that is why they particularly show up in T2 flair images so you can see it quiet clearly here.
Pia: You could also see it in T1 but yes.
Me: But now quiet as well, so you can see intensities here. Etc. Etc. And these are fairly clear white matter intensities as well.
Pia: Yes, but the McDonald....the McDonald criteria are not matched, ok.
There are no cervical or myelin lesions that we can see.
[the cervical and myelin lesions are gross and clearly apparent from a simple glance at the MRI, the doctors statement is a joke]
And then any radiologist sees.
[but there is gross evidence of radiological fraud to show clinicians intent]
So we have no oligoclonal bands. We have no....
[the test is fraud as described below in explicit detail]
Me: It appears that you have actually. You have actually preempted every single statement without actually looking at any of the medical reports.
Without actually, like, seeing all the images. You basically stated something preemptively without actually analyzing anything.
Pia: Im analyzing, im analyzing your.... the things that I read. I am analyzing the things that I see.
Me: These are also fairly significant things.
Pia: That's an EEG.
Me: Yea, this is an EEG. If there is an intensity in the posterior part of the brain. So the occipital lobe, you can also see it as sharp waves within that region of the brain. I can only argue in an intellectual sense.
I mean I cant argue just like you know......
Or you can see it..... Here is another way of showing that this is one series and I did another MRI series and I did another MRI series a month later and you can still see some lesions.
You can see some reduction in intensities, you can see how it improved form drug response.
Its not as well defined in this series. Etc. Etc..
These are sequential series from the same MRI Etc. Etc.
What I did, I did it as a scientific principal. I said we are going to test the condition using drug responses using the same MRI system, MRI machine.
We are going to do it redundantly and we are going to do see how it responds to the medication.
Pia: Ok, but you are not a doctor and you are not a neurologist. So it is my profession. I am a neurologist and as far as I see it, I question the diagnosis of multiple sclerosis.
[Under his profession Dr. Pia committed clear assault with an over abundance of evidence in doing so. This is Dr. Pia's delusion: though the patient had the condition and responds to the medications and has all the diagnostic data Dr. Pia tries to negate it with the statement, “you are not a doctor and you are not a neurologist”, which is absurd considering clinical history. I negated every statement by Dr. Pia as fraud as he was stating it with clear evidence of fraud]
Pia: Ok, we can admit you to our ward and another sort of testing. We can do the visual evoked potentials for example to see if you ever had an inflammation of the optical nerve.
[you wouldn't do a visual evoked potential to see if ”I ever had inflammation of the optical nerve” since it changes due to clinical severity, you would do a ophthalmologist test and a brain MRI of the optic nerve; hes making up clinical criteria]
We can do..... we can maybe think about.....
Me: Im not sure what the agenda behind this is. At this point this is a fairly typical presentation for me. I usually come to the ER when there is a massive of pain. Particularly.....
I mean these are cervical. This is cervical inflammation. So it will produce a particular type of headache and that is basically my presentation at this particular point.
That particular headache always responds to IV methylprednisolone.
So this was in IV. This was an ER appointment very much like this.
I went into the ER the neurologist did a full medical workup. She did all the blood tests. She did her neurotests and then she said this is how you present in the ER and given that, they actually applied the methylprednisolone at that point.
She looked at the MRIs. She readily stated these are T2 intensities in your CNS so you do actually need the methylprednisolone. So this was given in that particular ER instance.
And she said you readily have T2 intensities in both your brain and spine, it's a fairly direct reading because unless you are completely blind you can pretty much easily see it.
And then we did out IV methylprednisolone and then we did our neurotest
We can see the improvement in physiological stature and also reaction rate as well.
So this after 5 IVs and around 6 or 7 days and then we do a neurotest and then we can see the clinical improvement there.
And then what I did additively is that I did an MRI series after this IV series and you can see the improvement in the spinal column and also the brain as well.
So it becomes kind of a situation where the medication response is readily visible and its also visible in MRI series etc. etc.
Pia: In multiple sclerosis you have lesions.
Me: At his point.....
Pia: Ok, you have lesions but its not always inflammation of one lesion you have. You have no progress in terms of new lesions.
[Worlds most dimwitted and inappropriate statement in neurology, the object of medications is to prevent the formation of new lesions and further neurodegeneration. Dr. Pia's statement fits the asylum statement that the clinicals are withholding medication to physically/intellectually disfigure the patient. Which is exactly what Dr. Pia states, withholding medication to cause brain damage from MS to causing new lesions by medical neglect. Thus explicit assault by Dr. Pia as stated by Dr. Pia]
Me: I also take rebif as well, I try to manage. The point of MS is that no new lesions continue to form. That's why you take the medication.
[I stated it perfectly, the doctor's statement is counter to basic medical logic]
Pia: Well, you have two parts of medications. Ok. You have the acute medication. Methylpredniolone, ok. And then you have the basically medication you go and take to prevent new lesions.
Me: Rebif.
Pia: Which would be rebif for..... a thousand dollars so.... [?]
What did you say?
Me: Like 4 or 5 effective medications.
Pia: Well if you take the more modern ones its way more then 5, ok.
And since you have no progress, what so ever. Ok. You don't even....
We can do testing of course we can but I......
[Dr. Pia indicates intent of clinical malice, to harm the patient in clear statement by causing new lesions. Thus assault by Dr. Pia's own statement]
Me: Im not sure but coming into the ER. This actually qualifies as a bit of a relapse at this point. So im not sure....
Pia: If not, if you question the whole guidelines.....
Me: Yea, its not like.... At this point I only look for the drug response. And the drug response from methylprednisolone, it sticks. If you give the methylprednisolone IV, the automatic improvements doesn't last of a week, it doesn't last for two weeks it lasts for 4 and a half weeks at least.
So it reduces inflammation, it's a high dose. Its high dose for a particular reason. Its high dose particularly to effect your central nervous system.
At that point there is a symptomatic improvement for a period of time so the drug effectiveness is see in that instance.
I was luck enough to have access to a university level MRI at 3 tesla to see is it really reducing inflammation in the brain and I showed that as well.
Huh, and I went out and did the MRI and the condition presented itself again if in my case it will take another.....
Pia: But you know what an placebo effect is again.
Me: No not at all, not in this sense because I have no physical feeling in my hands my fingers my legs.
Pia: But you know what an placebo effect is. Can you, can you, can you tell me what a placebo effect it.
[Its clear to see that Dr. Pia is extremely aggressive and somewhat dimwitted. I had just then stated that I used MRIs to determine drug response as not being placebo. He defines intent in clinical neglect perfectly. The condition was shown to be secondary progressive MS with progressive neurological damage to spine and brain with all the surrounding diagnostics and MRIs to substantiate it inclusing MRIs to show drug response]
Me: I can tell with, I can also tell with cervical neuroinflammation in....
Pia: Please just lay down here.
Just take of your jacket and your shoes......
Me: This is an attempt at an somewhat intelligent argument but it still fails me because you know.
Pia: No, its just im being rational and when being rational I just have to question. Because I don't see..... I see no progress. I see not a form of a certain criteria fulfilled. We have no oligoclonal bands.
[I state that Dr. Pia is nonsensical and appropriately stated, Dr. Pia is neither rational nor did anything he say indicate anything other then intent to harm the patient. Combining this evidence with former evidence of radiological fraud indicates criminal intent in assault. Criteria was fulfilled a decade ago but radiological fraud combined with laboratory fraud means criminal intent to harm the patient. Dr. Pia is a police case for assault by definition. His rationality is centered around clinical harm to the patient while hiding disease pathology with easy proof and evidence]
Me: You could be rational to to support a very.... how do I say it.... not a good things to do to a person as well. Its an introverted kind of thing but like.
Pia: Well but let me you, I will give you your computer back. The thing is of course you have to question if you don't have the feeling that its right. Ok.
[all his statements indicate a somewhat deluded mentality]
Me: Yea.
Pia: And just giving you medication without the ground work and without the basis you are convinced of it being fulfilled. That.. then I would not be a good doctor. Ok. I will be back, I will be back in just a minute.
[deluded statements by Dr. Pia; hes using clinical fraud when the patient has the groundwork for the condition; repeatedly states intent in assault and cites two instances of clinical fraud to uphold assault]
Using radiological fraud in another setting to demonstrate the clinical fraud in Charity Hospital:
The falsification in Schumacher's statement can be determined by the evidence of fraud in another setting (the fraud takes place on January 10th 2017 in Riga, Latvia). This is the presentation of fraud in another setting and it pertains to how a radiologist tries to hide medical data by erasing sections of a MRI that shows a disease pathology.
The video of the clinical radiological fraud in this link:
https://narenjana.com/police/germany/mrifraud
negates Dr. Pia Schumacher is this way:
1. 1. The criteria for MS was fulfilled a decade ago before but evidence of lesions were erased, hidden, or with false reports to not mention them. Thats repeated clinical fraud to intentionally try to harm the patient.
2. 2. There are central lesions in the MRI series which the radiologist identifies and hides. By hiding it the radiologist revels the location of the central lesions and the intent of both the radiologist and the Dr. Pia Schumacher. These are demyelination lesions typical of MS (which Dr. Pia mentions) The MRIs looked at by Dr. Pia have gross central lesions but were attempted to be hidden by former radiologists.
3. 3. The central lesion evolves to neurodegeneration, which Dr. Pia Schumacher tries to misstate as "disk" degeneration of the spine, which is aburd. It's a central region of demyelination that evolves to neurodegeneration of the spinal cord. The radiologist is trying to hide progress in the clinical condition and Dr. Pia Schumacher is harming the patient by trying to create new lesions to create progress to physical disable the patient:
So since there is clear evidence of fraud in one setting that evidence of fraud is also easy to apply to the falsified statement of Dr. Pia Schumacher. What is stated by Dr. Schumacher as "protrusions" or "disk" degeneration are really a features of neurodegeneration intentionally mistated by Dr. Schumacher to perpetuate medical neligence and assault in this medical setting.
These features of neurodegeneration only occur from repeated inflammatory episodes (due to multiple sclerosis) that take place in the central spinal canal (which is what the radiologist in this video is trying to hide) not the skeletal system. These features only occur due to long term neurodegeneration from long term conditions like progressive Multiple Sclerosis. I have progressive multiple sclerosis.
This combined with the fraud of the LP test in Charity hospital there is an over abundance of evidence to demonstrate assault by the clinical with the intent of harming the patient. The surrounding evidence of fraud in the LP test is given here:
https://narenjana.com/police/germany/labfraud
Its simply a direct example of fraud in a medical setting with an attempt to repeat that same clinical fraud in another setting. Dr. Pia's statements are clinical fraud substantiated by clinical fraud in another setting with clear evidence (MRI and Lab fraud).
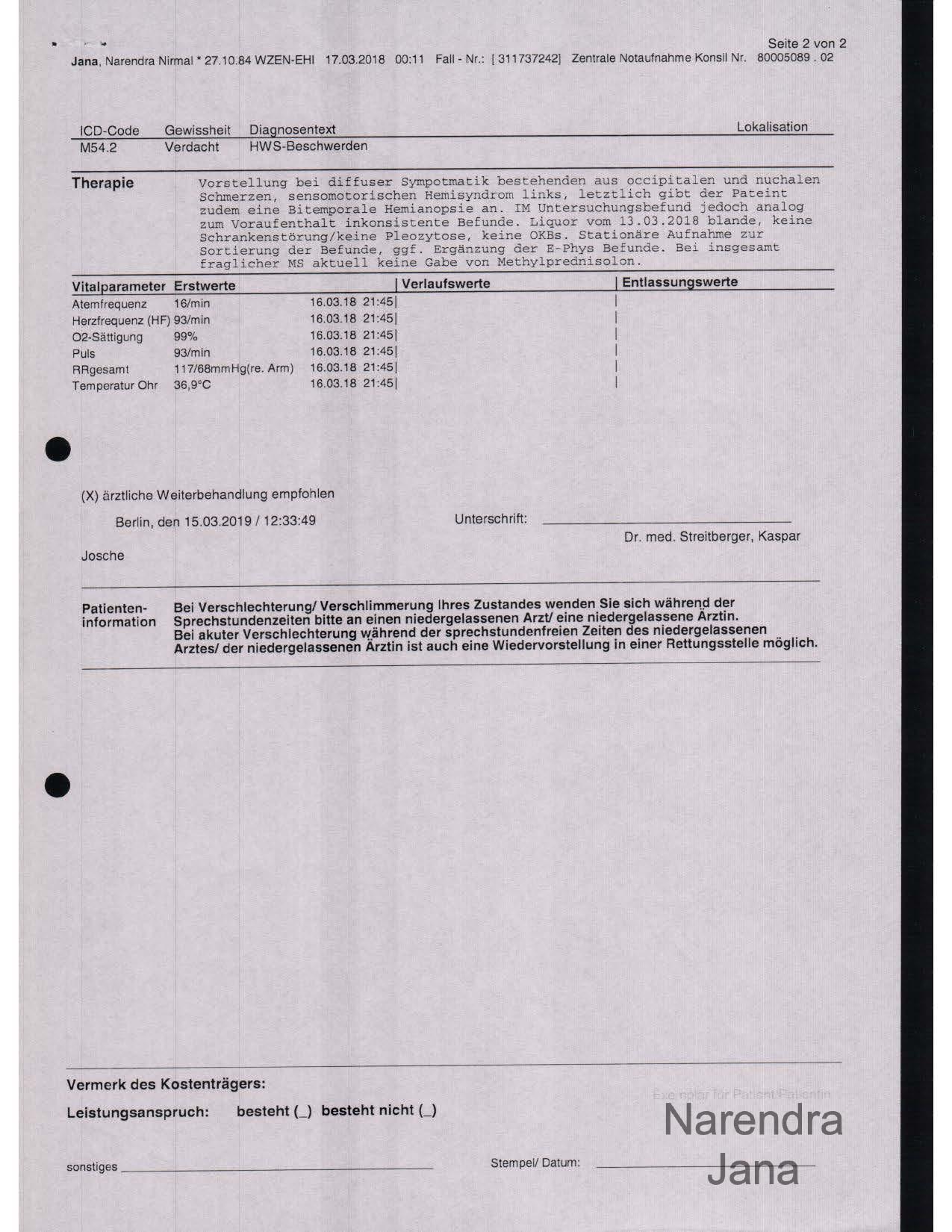
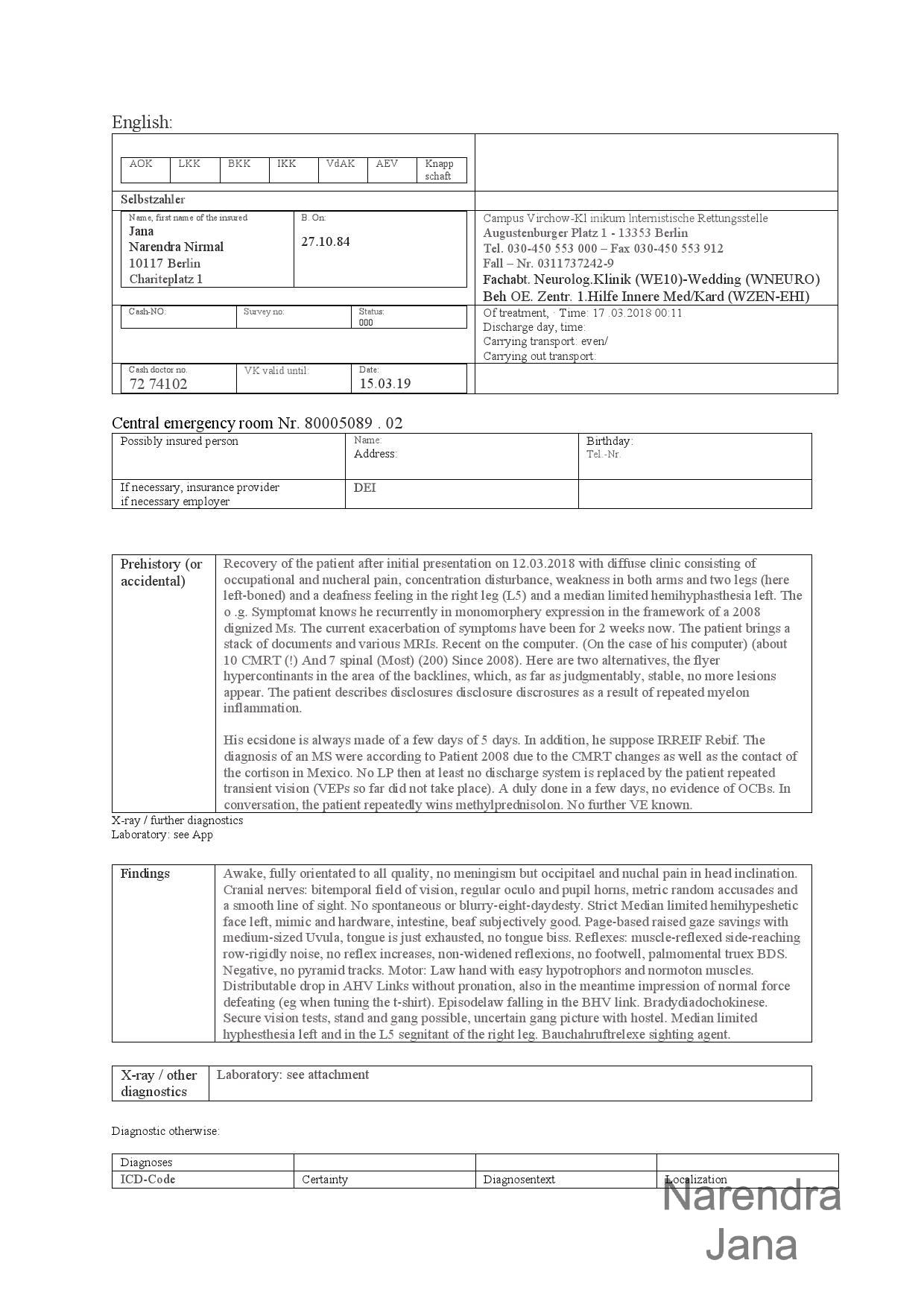
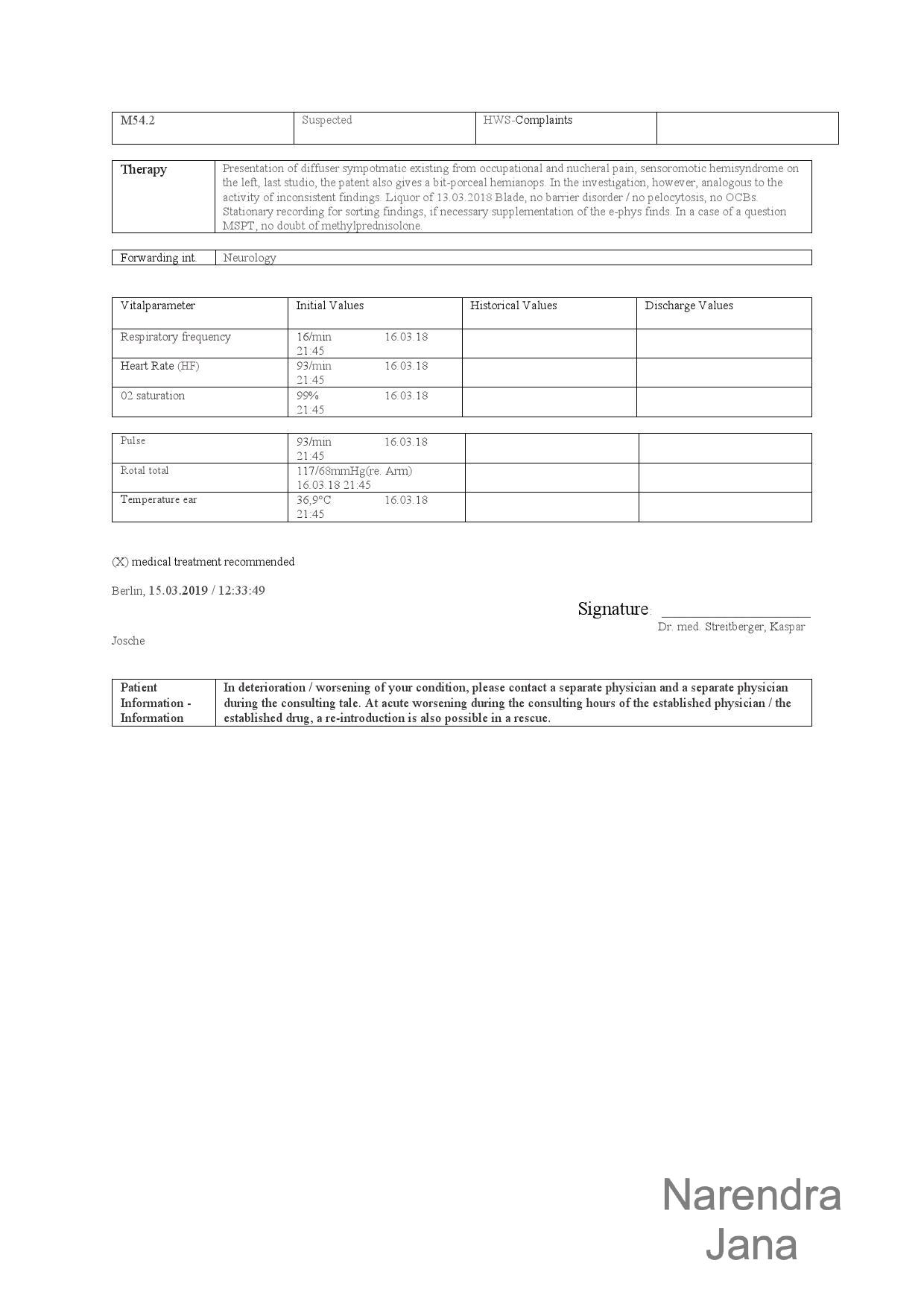
Discharge Report (Dr. Kaspar Streitberger) from March 17th 2018 Charity Virchow:
|
|
|
|
|
Clinical Condition on March 17th Charity Virchow Ward where medications arent Given is Shown Below:
|
How the clinical condition evolved in recent clinical setting on April 13th 2020 is given below (another instance of assualt in a clinical setting that perpetuates the statuate of former instances of assualt):
|
This demonstrates why the medications were needed in the past and how it progressed the condition to recent presentation. Thus Charity Hospital's denial of medical help is assault by both recent and past evidence.
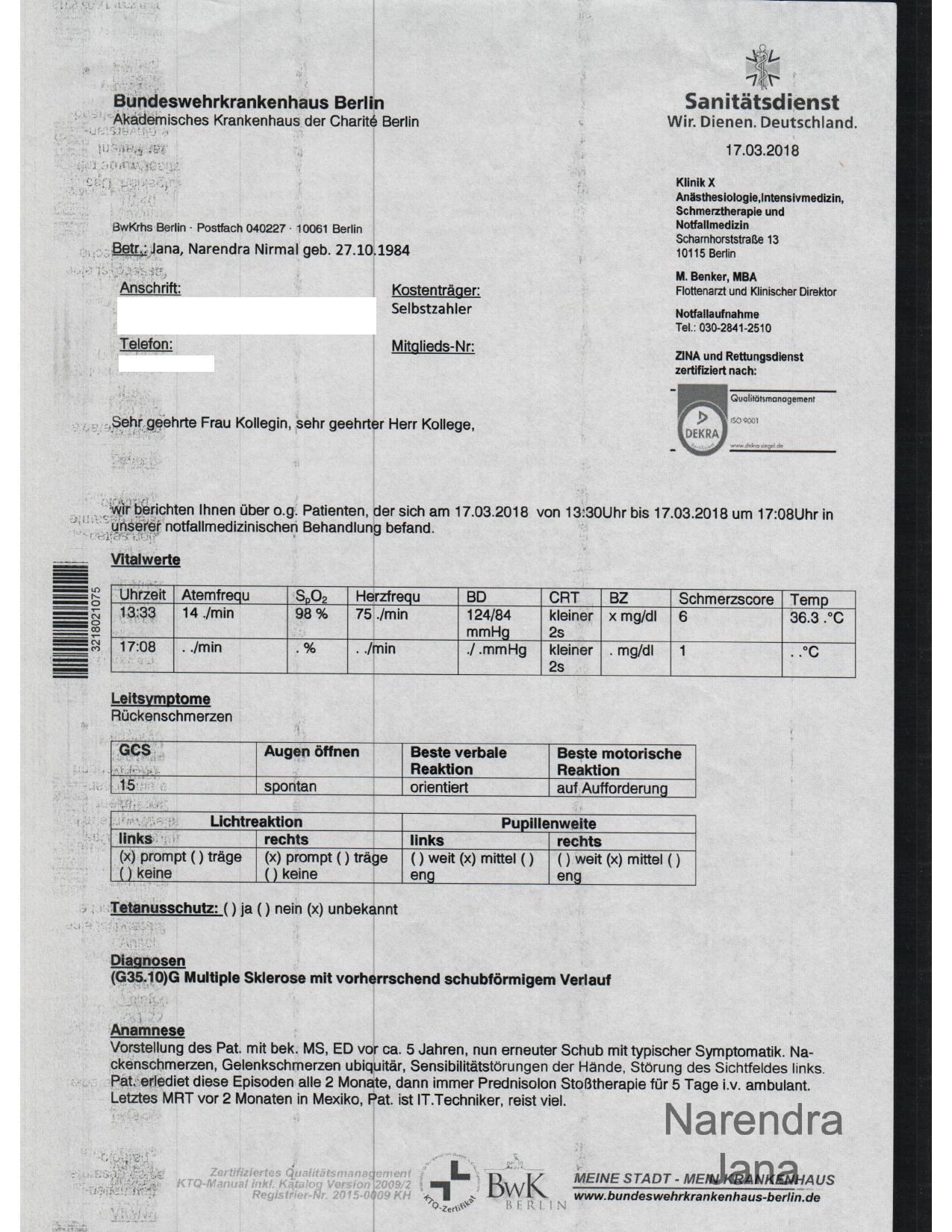
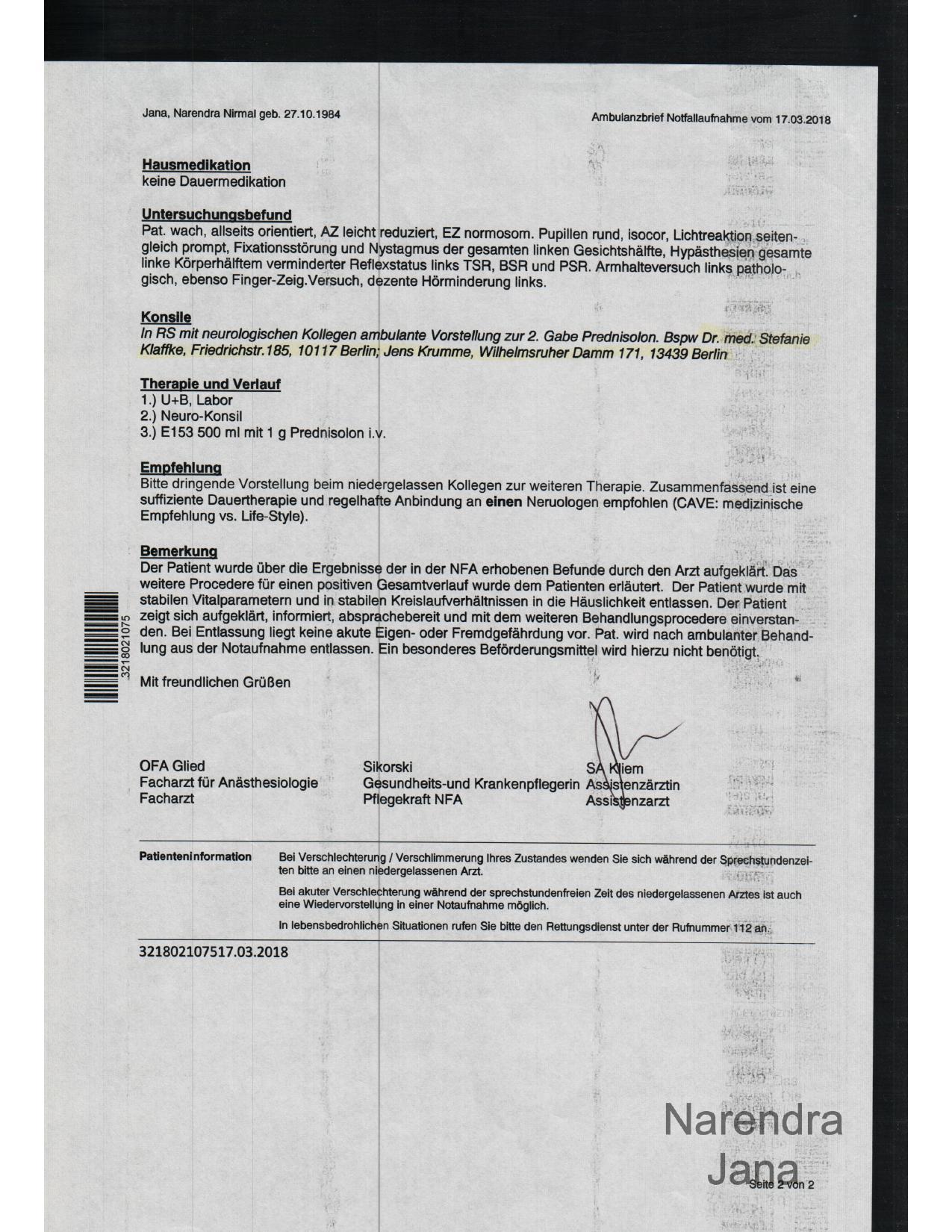
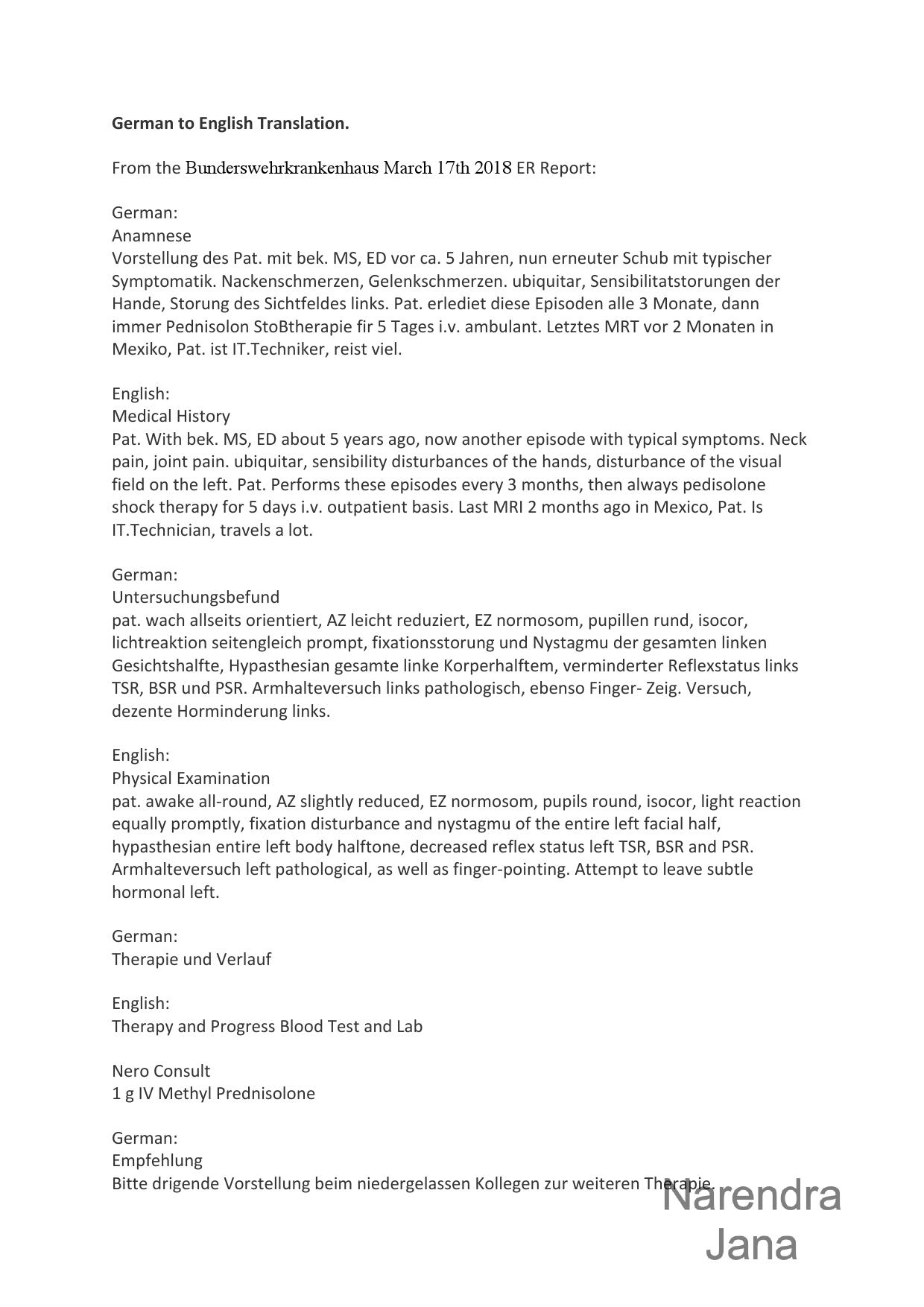
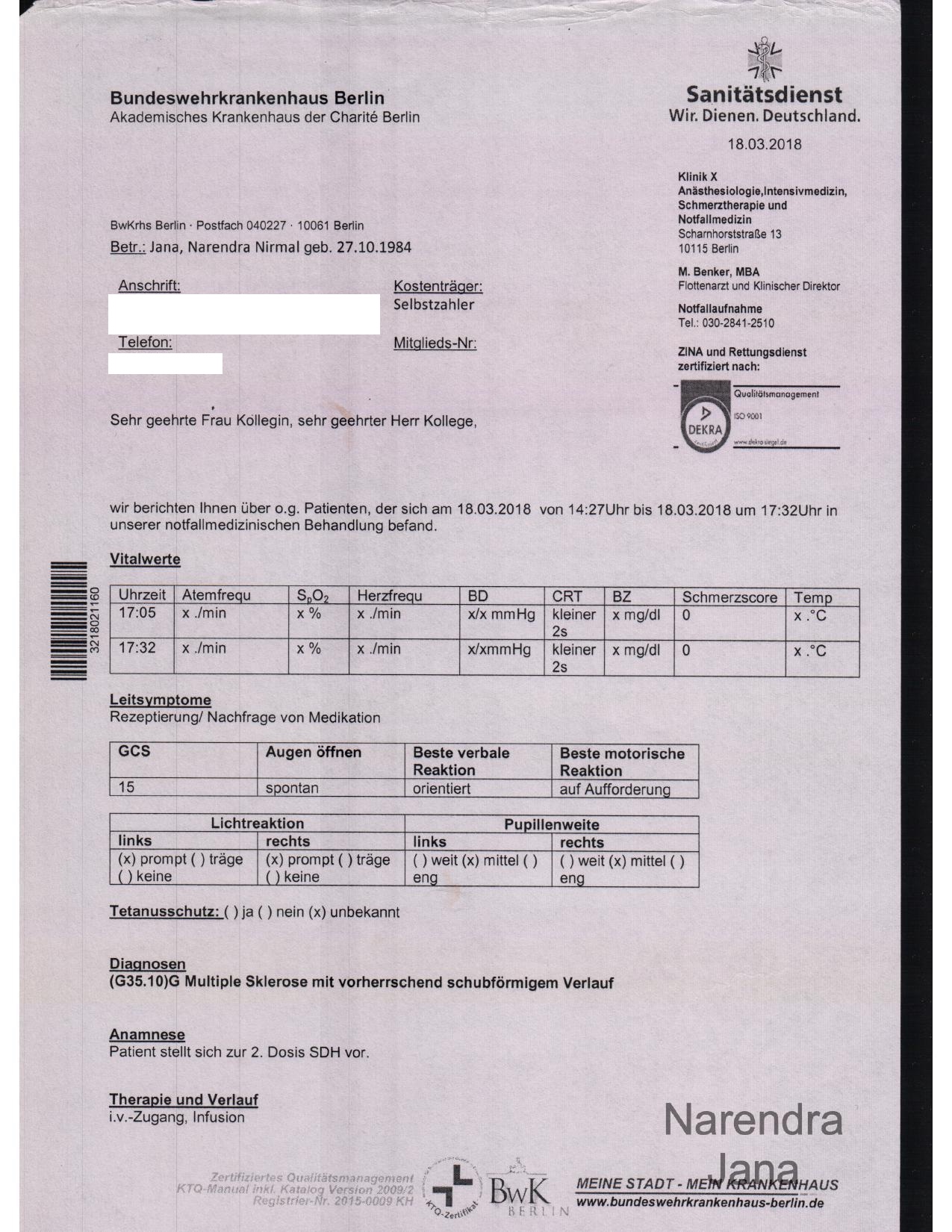
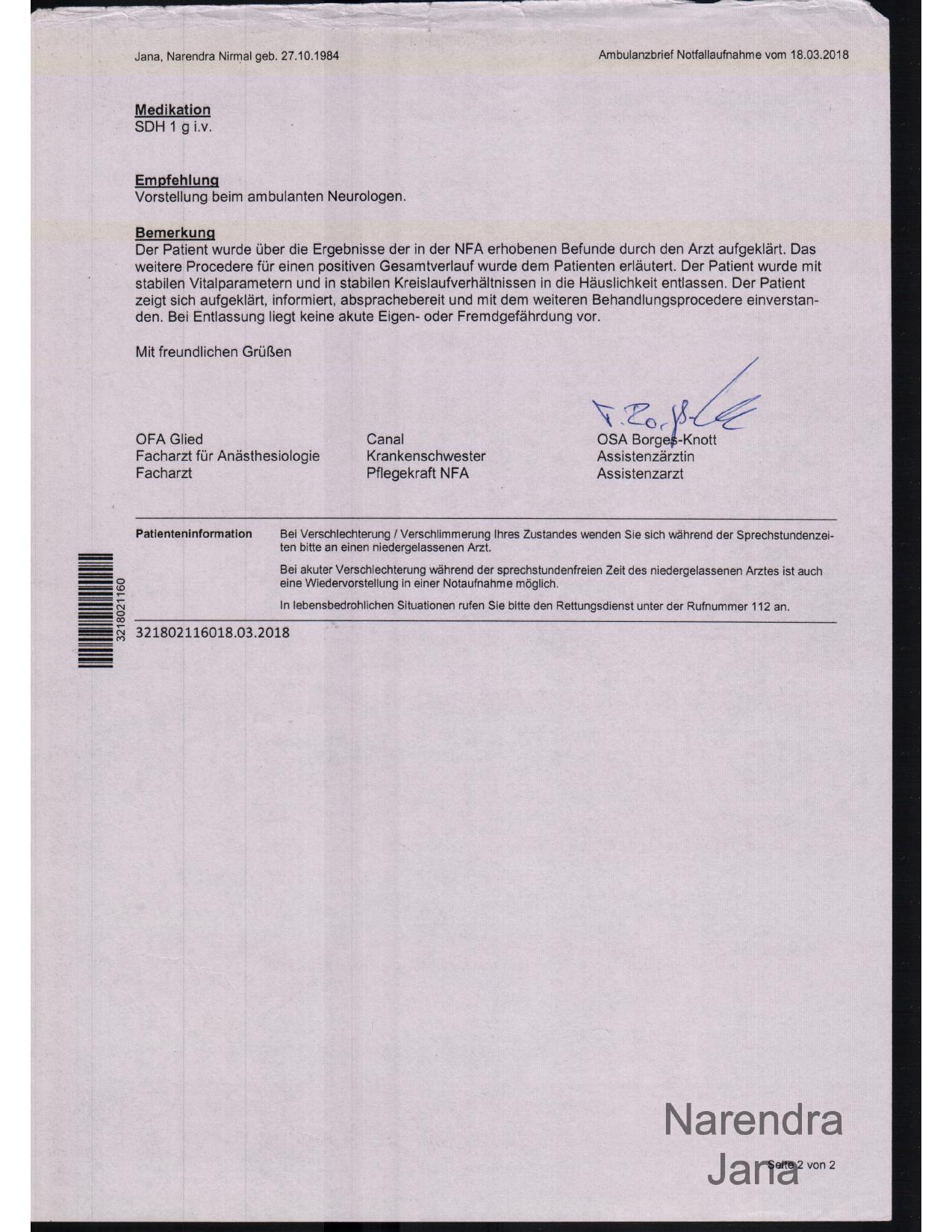
Clinical Condition on March 17th in Bunderswehrkrankenhaus Berlin where medications are Given to a Positive clinical effect is shown below:
March 17th 2018 Bunderswehrkrankenhaus Berlin immediately after Leaving Charity Virchow (where medications are given):
|
|
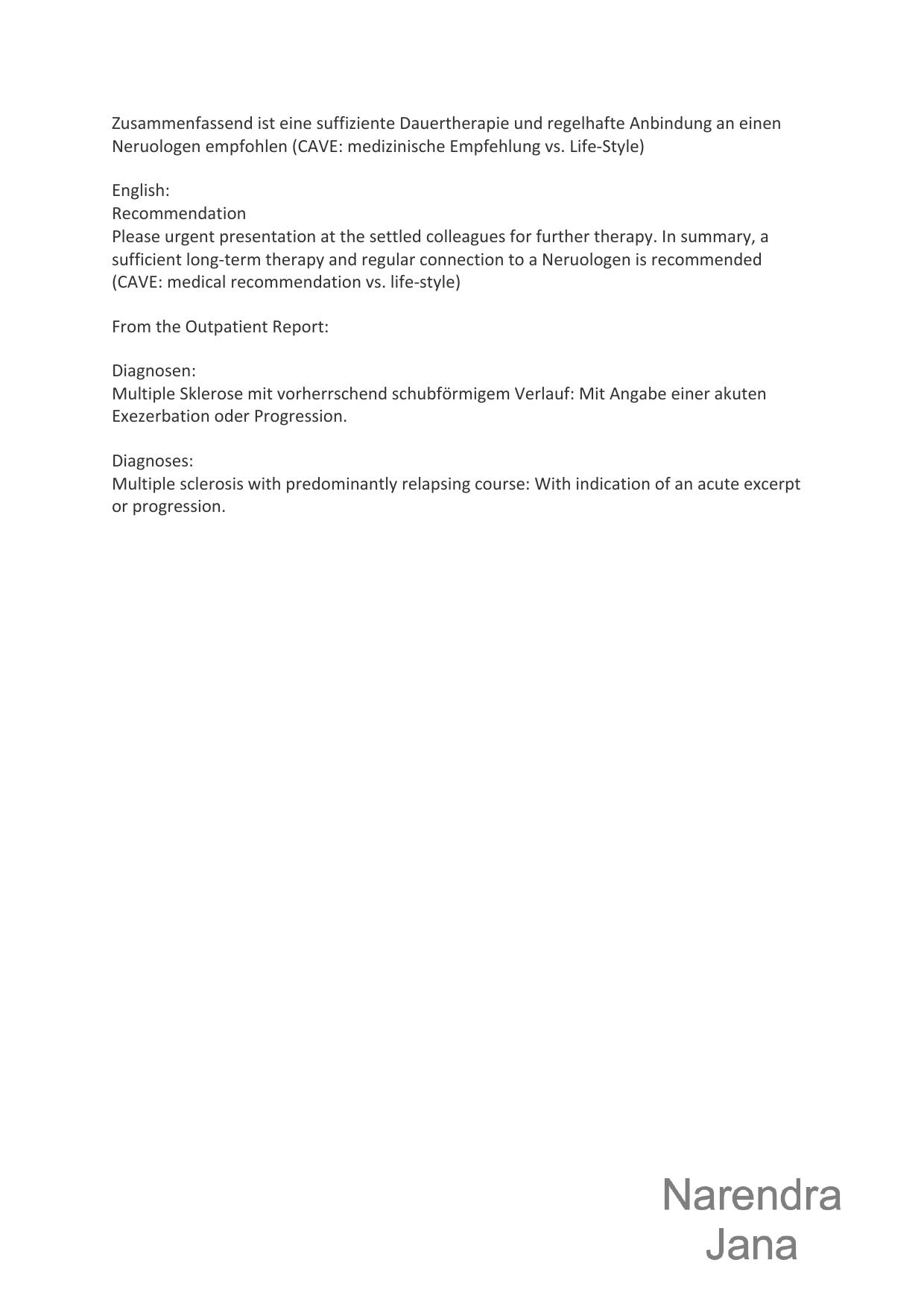
English Translation is given below:
|
|
|
|
|
Blood Test Result from Bunderswehrkrankenhaus Berlin: 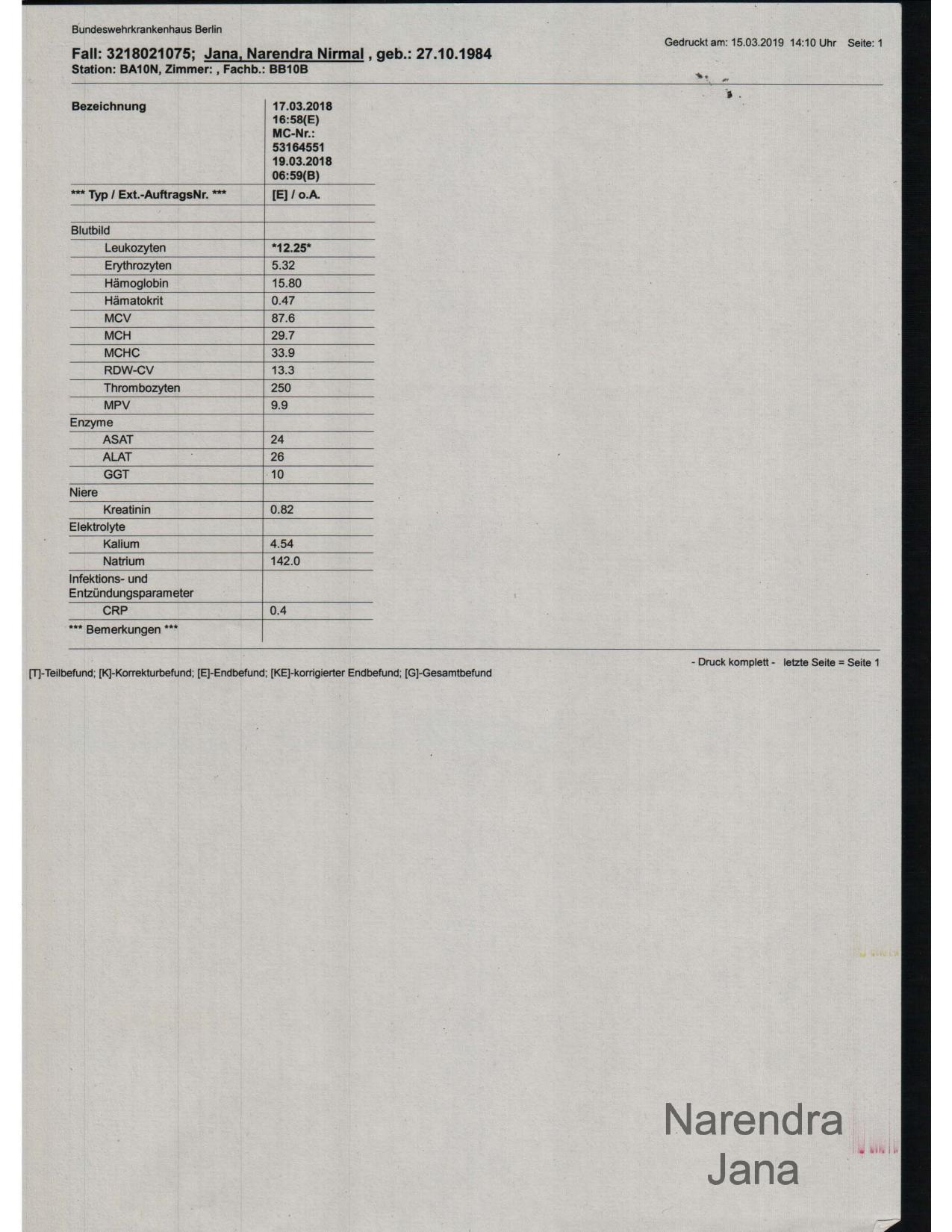
|
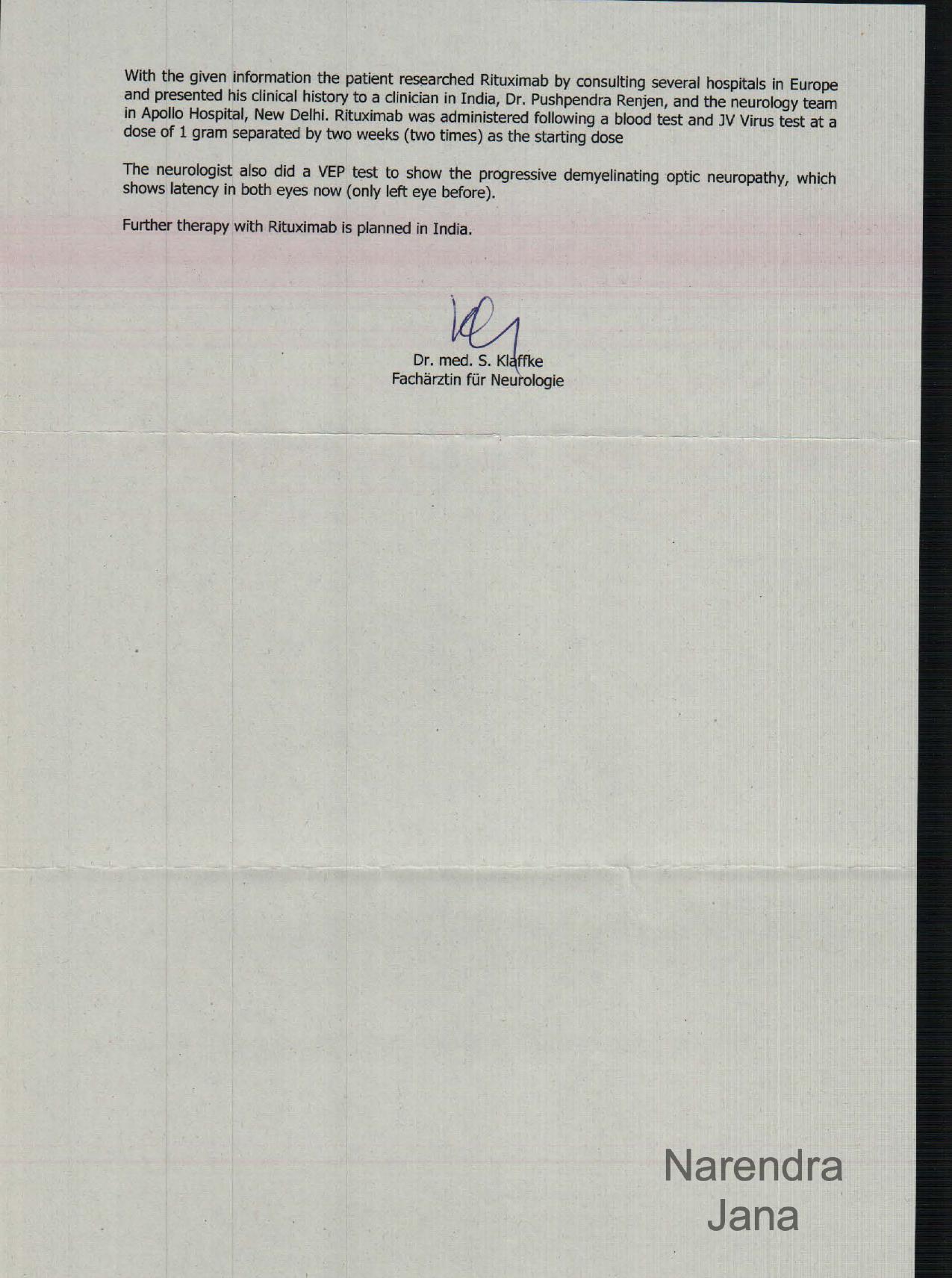
Dr. med. Stefanie Klaffke's clinical summary describing my 3 day IV continuation after Bunderswehrkrankenhaus is given below. It also described a part of my clinical history after the ER and how I have secondary progressive Multiple Sclerosis:
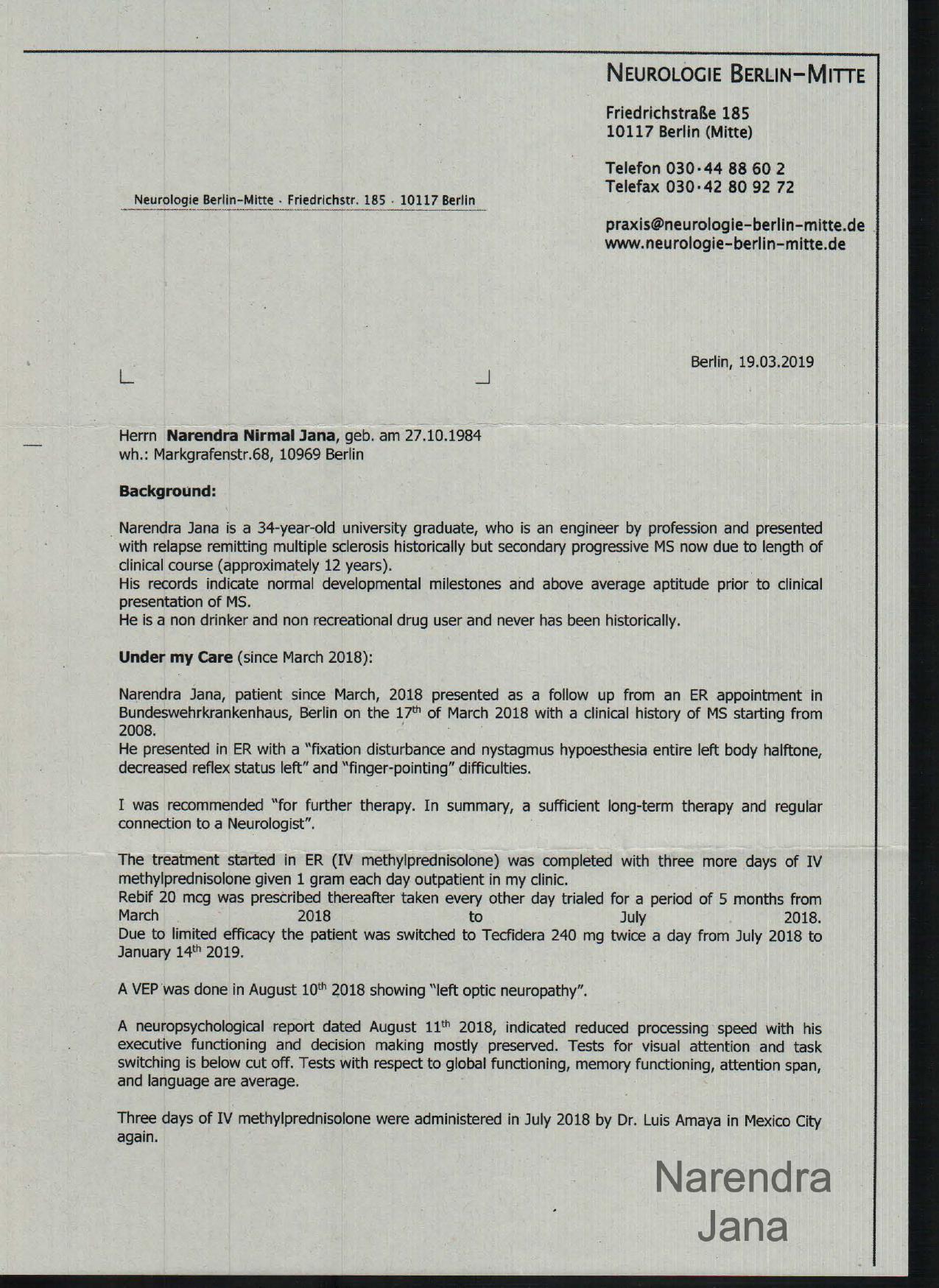
|
|